Pit and fissure sealants
The occlusal morphology of the posterior teeth comprises of pits and fissures which are more prone to plaque accumulation in comparison to smooth surfaces. Difficulty in maintaining oral hygiene is another attribute that increases susceptibility of dental caries in them.
It has been noted that the enamel in pit and fissures does not receive the same level of caries protection from fluoride as smooth surface hence, it is important to protect these vulnerable sites.
Sealant application is a preventive dental treatment in which the application of sealants into pits and fissures forms a micromechanical bond with the tooth thus providing a physical barrier that keeps bacteria away from their source of nutrient.
Occlusal morphology of fissures:
Indication for sealants depends on the morphology of fissures. Commonly seen patterns are-
| V type: | shallow and wide, tend to be self-cleaning and somewhat caries-resistant | non-invasive technique is recommended |
| U-type: | shallow and wide, tend to be self-cleaning and somewhat caries-resistant | non-invasive technique is recommended |
| I-type: | deep, narrow, and quite constricted, resembling a bottleneck, caries susceptible | may require invasive technique |
| IK- type: | narrow slit associated with a larger shape at the bottom, highly susceptible to caries | may require invasive technique |
Where to place sealants:
1. Pit and fissure of primary or permanent teeth when the patient is at a high risk of experiencing caries
2. Non-cavitated deep pits and fissures in children, adolescents, and adults
3. Individuals with special health care needs
Where not to place sealants:
1. Shallow self-cleansing fissures in primary or permanent teeth
2. Patients with low risk of developing carious lesion
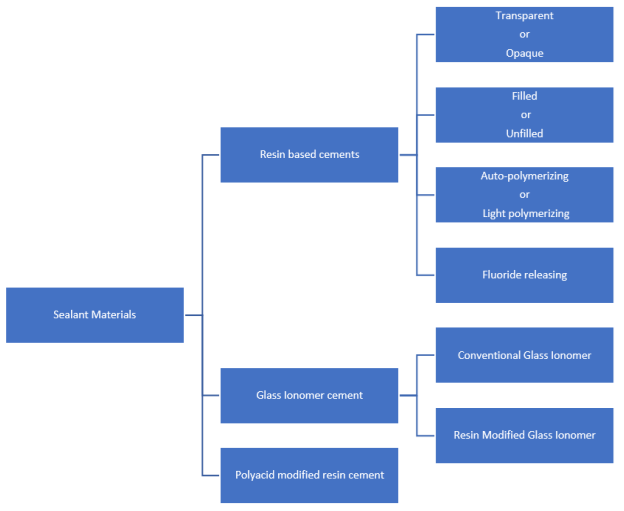
Classification: Pit and Fissure Sealant Materials are classified into three main types:
Procedure for sealants placement:
It is suggested to clean the tooth with prior sealant application with pumice or air polishing to ensures better etching. Isolate the tooth using rubber dam as moisture control is important for the success of sealants. In newly erupted teeth a dry field can be achieved by cotton rolls and isolation shields. The tooth is etched using 37% orthophosphoric acid gel using application tips or brush. Enamel is etched for 15 seconds for permanent molars and 15 to 30 seconds for primary teeth. Teeth with dental fluorosis require additional etching time than this. Teeth are water sprayed and air dried to get a frosty white appearance. Following this bonding agent is applied and cured.
If glass ionomer cement is being used, etching and adhesive is not required, and a surface conditioner may be used. Sealant is made to flow from distal to mesial side in mandibular teeth and from mesial aspect to distal in maxillary teeth. Material should flow till cuspal inclines. It is then cured for 10 to 20 seconds using visible light. Sealant placement should be evaluated visually as well as clinically. If the sealant has been lost or partially retained, it should be reapplied.
Follow up appointments are required for clinically and radiographical monitoring.
Adhesive System:
• A systematic review compared the retention rate of sealants, combined with self-etch adhesive systems (sixth or seventh generation), with that of etch-and-rinse adhesive systems (fourth and fifth generations). The systematic review concluded that the retention of occlusal fissure sealants is higher when applied with the etch-and-rinse adhesive system than with the self-etch adhesive system.
• An evidence-based report from the American Dental Association and the American Academy of Pediatric Dentistry supports the use of adhesive systems before sealant application for better sealant retention.
Reasons for failure:
Most common cause is due to contamination from either saliva or calcium phosphate products. Incomplete or slow photopolymerization, air entrapment during placement are few other causes.
Controversies:
• Bisphenol-A (BPA) are the most common monomers used in resin composite restorations and resin-based sealants. It is known for its estrogenic property with potential reproductive and developmental human toxicity. However, American Association of Pediatric Dentistry Guidelines, the US Drug and Food Administration (FDA), and the American Dental Association have concluded that the low-level of BPA exposure from dental sealants poses no known health risks.
• There were concerns about partially lost sealant in that it may leave sharp margins that trap food and eventually lead to caries. A systematic review evaluated if the risk of developing caries in previously sealed teeth with fully or partially lost sealant surpasses the risk in teeth that have never been sealed. It was found that the risk of caries development in previously sealed teeth after a four-year follow-up is less than or equal to that for never-sealed teeth. In other words, teeth with partial or complete sealant loss are not at a higher risk of developing caries compared to never-sealed teeth.
Conclusion:
Selection of sealant material depends on various factors like affordability, patient’s age, isolation technique and the time of teeth eruption. Caries risk assessment is also important in the decision-making process. With periodic recall and evaluation, sealant is an effective means of preventing pit and fissure caries in primary and permanent teeth.
References:
1.Griffin, S.O.; Gray, S.K.; Malvitz, D.M.; Gooch, B.F. Caries risk in formerly sealed teeth. J. Am. Dent. Assoc. 2009, 140, 415–423. [CrossRef] [PubMed]
2. Rohr M, Makinson OF, Burrow MF. Pits and fissures: morphology. ASDC J Dent Child. 1991 Mar-Apr;58(2):97-103
3. Botton, G.; Morgental, C.S.; Scherer, M.M.; Lenzi, T.L.; Montagner, A.F.; Rocha, R.D.O. Are self-etch adhesive systems effective in the retention of occlusal sealants? A systematic review and meta-analysis. Int. J. Paediatr. Dent. 2015, 26, 402–411. [CrossRef] [PubMed]
4. Beauchamp, J.; Caufield, P.W.; Crall, J.J.; Donly, K.; Feigal, R.; Gooch, B.; Ismail, A.; Kohn, W.; Siegal, M.; Simonsen, R. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: A report of the American Dental Association Council on Scientific Affairs. J. Am. Dent. Assoc. 2008, 139, 257–268. [CrossRef] [PubMed]